Summary: Researchers report a procedure that wipes out the immune system and then regenerates a new one using stem cells may effectively eliminate all signs of neuroinflammation in people with early, aggressive MS.
Source: Ottawa Hospital Research Institute.
Clinical trial suggests chemo and blood stem cell combination therapy should be considered for people with early, aggressive MS.
A clinical trial published in The Lancet, a top medical journal, shows that an intensive procedure that completely wipes out the immune system and then regenerates a new one using blood stem cells can eliminate all signs of damaging brain inflammation in people with early, aggressive multiple sclerosis (MS), and facilitate lasting recovery.
Led by Dr. Harold Atkins and Dr. Mark S. Freedman of The Ottawa Hospital and the University of Ottawa, the trial included 24 participants who were followed for up to 13 years. The $6.47 million trial was funded by the MS Society of Canada and its affiliated Multiple Sclerosis Scientific Research Foundation. The research was also supported by The Ottawa Hospital Foundation, The Ottawa Hospital Department of Medicine and Canadian Blood Services.
“Our trial is the first to show the complete, long-term suppression of all inflammatory activity in people with MS,” said Dr. Atkins, a stem cell transplant physician and scientist at The Ottawa Hospital, and associate professor at the University of Ottawa. “This is very exciting. However, it is important to note that this therapy can have serious side effects and risks, and would only be appropriate for a small proportion of people with very active MS. People with MS who have had significant disability for a long time would likely not benefit.”
“This procedure should be considered as a treatment option for people with early, aggressive MS,” said Dr. Freedman, a neurologist and senior scientist at The Ottawa Hospital and professor at the University of Ottawa. “Although this trial was relatively small, it was intensive, with the longest prospective follow-up of any such treatment group to date, and that is what makes the results so convincing. However, this is a very complex procedure that should only be performed at very specialized centres with expertise in both the management of MS patients and blood stem cell transplantation.”
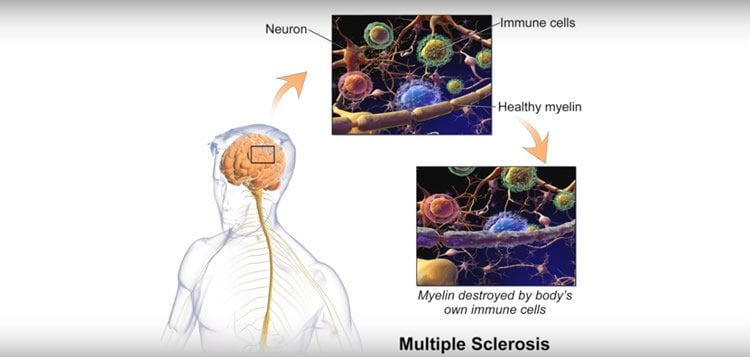
MS affects approximately 2.3 million people around the world, causing symptoms that range from blurred vision to extreme fatigue to partial or complete paralysis. It occurs when the immune system – which normally protects against foreign disease-causing organisms – mistakenly attacks the body’s own central nervous system, which includes the brain, spinal cord and optic nerve. Early in the disease, people often experience temporary episodes of worsening symptoms accompanied by active inflammation in the brain (called relapses), whereas later on, disease progression is inevitable.
The trial evaluated a treatment called immunoablation and autologous hematopoietic stem cell transplantation (IAHSCT). The procedure begins by giving a person medication to coax their hematopoietic stem cells to migrate from their bone marrow into their blood. These stem cells are then collected from the blood, purified and frozen. Then, high doses of chemotherapy drugs are used to eliminate the person’s diseased immune system. The stem cells are then transplanted back into the same person, so that they can give rise to a new immune system that has no “memory” of the previous pattern of attacking the central nervous system.
The trial included 24 participants with aggressive, relapsing MS. They were followed for anywhere between four and 13 years after treatment (with a median post-treatment follow up of 6.7 years).
After the treatment:
- Not a single participant experienced a clinical relapse (zero relapses in 179 patient-years), whereas before treatment, the participants experienced an average of 1.2 relapses per year (167 relapses in 146 patient-years).
- Not a single new active inflammatory lesion could be detected in the brains of any of the participants (zero lesions on 327 MRI scans) whereas before the treatment, participants had 188 lesions on 48 scans.
- Not a single participant required MS-specific drugs to control their disease.
- 70 percent of participants experienced a complete stop in disease progression.
- The average rate of brain shrinkage, typically a measure that correlates with MS progression, returned to levels associated with normal aging.
- 40 percent of participants experienced some lasting reversal of symptoms such as vision loss, muscle weakness and balance problems.
Some participants were able to return to work or school, regain the ability to drive, get married and have children.
Trial participant Jennifer Molson was diagnosed with MS in 1996, when she was just 21. She received her transplant in 2002.
“Before my transplant I was unable to walk or work and was living in assisted care at The Ottawa Hospital Rehabilitation Centre,” she said. “Now I am able to walk independently, live in my own home and work full time. I was also able to get married, walk down the aisle with my Dad and dance with my husband. I’ve even gone downhill skiing. Thanks to this research I have been given a second chance at life.”
“The MS Society is proud to be a part of an important turning point in the treatment of MS,” said Yves Savoie, CEO and President of the MS Society of Canada. “What started as a bold idea has translated into a treatment option for people living with highly active, relapsing MS. Publication of the results from this study will inform clinicians of the risks and benefits of the procedure, and pave the way for further research which could help people with all forms of MS.”
“A variation of this procedure has been used to treat leukemia for decades, but its use for auto-immune diseases is relatively new,” said Dr. Atkins, who is also the Medical Director of the Regenerative Medicine Program at the Ottawa Hospital Research Institute. “It is only used in very severe cases because participants face a significant risk of infection and other side-effects, including death. The risks are similar to those faced by leukemia patients undergoing this kind of treatment.”
A clinical trial published in The Lancet, a top medical journal, shows that an intensive procedure that completely wipes out the immune system and then regenerates a new one using blood stem cells can eliminate all signs of damaging brain inflammation in people with early, aggressive multiple sclerosis (MS), and facilitate lasting recovery.
Indeed, one participant in this study died of liver failure due to the treatment and another required intensive care for liver complications. The treatment regimen was modified over the course of the study to reduce toxicity, but all participants still developed fevers, which were frequently associated with infections.
“Several recent clinical trials from other groups have examined this procedure in people with MS,” said Dr. Freedman, who is also the Director of MS Research at The Ottawa Hospital. “Our study is unique in that we used a stronger cocktail of drugs to eliminate the immune system, we followed the participants for a very long time, and the majority of our participants have had significant, long-lasting responses.”
People who are interested in this therapy should speak with their own neurologist, who can request a referral to The Ottawa Hospital MS Clinic or another major hospital with experience in this area. Note that The Ottawa Hospital cannot treat people without valid Canadian health coverage.
This study was approved by the Ottawa Health Sciences Network Research Ethics Board, and is registered at https://clinicaltrials.gov/ct2/show/NCT01099930. The lead researchers are affiliated with the Stem Cell Network, the Ontario Institute for Regenerative Medicine and the University of Ottawa Brain and Mind Research Institute.
“We thank the patients from across Canada who participated in this clinical trial, as well as their family members,” said Marjorie Bowman, trial coordinator and advanced practice nurse at The Ottawa Hospital. “Their courage and dedication are remarkable.”
Funding: The study was funded by MS Society of Canada, Multiple Sclerosis Scientific Research Foundation, Ottawa Hospital Foundation, Ottawa Hospital Department of Medicine, Canadian Blood Services.
The authors declare no relevant conflicts of interest.
Source: Deirdre Branley – Ottawa Hospital Research Institute
Image Source: This NeuroscienceNews.com image is adapted from the Ottawa Hosptial video.
Video Source: Video is credited to Ottawa Hospital.
Original Research: Abstract for “Immunoablation and autologous haemopoietic stem-cell transplantation for aggressive multiple sclerosis: a multicentre single-group phase 2 trial” by Dr Harold L Atkins, MD, Marjorie Bowman, MScN, David Allan, MD, Grizel Anstee, MD, Prof Douglas L Arnold, MD, Prof Amit Bar-Or, MD, Isabelle Bence-Bruckler, MD, Paul Birch, MLT, Prof Christopher Bredeson, MD, Jacqueline Chen, PhD, Prof Dean Fergusson, PhD, Mike Halpenny, MLT, Linda Hamelin, RN, Prof Lothar Huebsch, MD, Brian Hutton, PhD, Pierre Laneuville, MD, Yves Lapierre, MD, Hyunwoo Lee, BSc, Lisa Martin, MLT, Sheryl McDiarmid, RN, Prof Paul O’Connor, MD, Timothy Ramsay, PhD, Mitchell Sabloff, MD, Lisa Walker, PhD, and Prof Mark S Freedman, MD in The Lancet. Published online June 2016 doi:10.1016/S0140-6736(16)30169-6
[cbtabs][cbtab title=”MLA”]Ottawa Hospital Research Institute. “Standard Blood Pressure Target is Suffiecient for Treating Some Strokes.” NeuroscienceNews. NeuroscienceNews, 10 June 2016.
<https://neurosciencenews.com/ms-immune-system-progress-repair-4431/>.[/cbtab][cbtab title=”APA”]Ottawa Hospital Research Institute. (2016, June 10). Standard Blood Pressure Target is Suffiecient for Treating Some Strokes. NeuroscienceNews. Retrieved June 10, 2016 from https://neurosciencenews.com/ms-immune-system-progress-repair-4431/[/cbtab][cbtab title=”Chicago”]Ottawa Hospital Research Institute. “Standard Blood Pressure Target is Suffiecient for Treating Some Strokes.” https://neurosciencenews.com/ms-immune-system-progress-repair-4431/ (accessed June 10, 2016).[/cbtab][/cbtabs]
Abstract
Immunoablation and autologous haemopoietic stem-cell transplantation for aggressive multiple sclerosis: a multicentre single-group phase 2 trial
Background
Strong immunosuppression, including chemotherapy and immune-depleting antibodies followed by autologous haemopoietic stem-cell transplantation (aHSCT), has been used to treat patients with multiple sclerosis, improving control of relapsing disease. We addressed whether near-complete immunoablation followed by immune cell depleted aHSCT would result in long-term control of multiple sclerosis.
Methods
We did this phase 2 single-arm trial at three hospitals in Canada. We enrolled patients with multiple sclerosis, aged 18–50 years with poor prognosis, ongoing disease activity, and an Expanded Disability Status Scale of 3·0–6·0. Autologous CD34 selected haemopoietic stem-cell grafts were collected after mobilisation with cyclophosphamide and filgrastim. Immunoablation with busulfan, cyclophosphamide, and rabbit anti-thymocyte globulin was followed by aHSCT. The primary outcome was multiple sclerosis activity-free survival (events were clinical relapse, appearance of a new or Gd-enhancing lesion on MRI, and sustained progression of Expanded Disability Status Scale score). This study was registered at ClinicalTrials.gov, NCT01099930.
Findings
Between diagnosis and aHSCT, 24 patients had 167 clinical relapses over 140 patient-years with 188 Gd-enhancing lesions on 48 pre-aHSCT MRI scans. Median follow-up was 6·7 years (range 3·9–12·7). The primary outcome, multiple sclerosis activity-free survival at 3 years after transplantation was 69·6% (95% CI 46·6–84·2). With up to 13 years of follow-up after aHSCT, no relapses occurred and no Gd enhancing lesions or new T2 lesions were seen on 314 MRI sequential scans. The rate of brain atrophy decreased to that expected for healthy controls. One of 24 patients died of transplantation-related complications. 35% of patients had a sustained improvement in their Expanded Disability Status Scale score.
Interpretation
We describe the first treatment to fully halt all detectable CNS inflammatory activity in patients with multiple sclerosis for a prolonged period in the absence of any ongoing disease-modifying drugs. Furthermore, many of the patients had substantial recovery of neurological function despite their disease’s aggressive nature.
Funding
Multiple Sclerosis Scientific Research Foundation.
“Immunoablation and autologous haemopoietic stem-cell transplantation for aggressive multiple sclerosis: a multicentre single-group phase 2 trial” by Dr Harold L Atkins, MD, Marjorie Bowman, MScN, David Allan, MD, Grizel Anstee, MD, Prof Douglas L Arnold, MD, Prof Amit Bar-Or, MD, Isabelle Bence-Bruckler, MD, Paul Birch, MLT, Prof Christopher Bredeson, MD, Jacqueline Chen, PhD, Prof Dean Fergusson, PhD, Mike Halpenny, MLT, Linda Hamelin, RN, Prof Lothar Huebsch, MD, Brian Hutton, PhD, Pierre Laneuville, MD, Yves Lapierre, MD, Hyunwoo Lee, BSc, Lisa Martin, MLT, Sheryl McDiarmid, RN, Prof Paul O’Connor, MD, Timothy Ramsay, PhD, Mitchell Sabloff, MD, Lisa Walker, PhD, and Prof Mark S Freedman, MD in The Lancet. Published online June 2016 doi:10.1016/S0140-6736(16)30169-6