

Summary: The famous rubber hand illusion may help people with OCD overcome their condition without the stress of exposure therapy.
Source: University of Cambridge
Obsessive compulsive disorder (OCD) affects as many as one in 50 people worldwide. One of the most common types of the condition, affecting almost a half of OCD patients, is characterised by severe contamination fears – even from touching something as commonplace as a door knob – leading to excessive washing behaviour. The condition can have a serious impact on people’s lives, their mental health, their relationships and their ability to hold down jobs.
OCD is treated using a combination of medication such as Prozac and a form of cognitive behavioural therapy (‘talking therapy’) termed ‘exposure and response prevention’. This exposure therapy often involves instructing OCD patients to touch contaminated surfaces, such as a toilet, but to refrain from then washing their hands; however, this experience can be so stressful that many patients cannot take part.
“OCD can be an extremely debilitating condition for many people, but the treatments are not always straightforward,” explained Baland Jalal, a neuroscientist based in the Department of Psychiatry at the University of Cambridge. “In fact, exposure therapy can be very stressful and so is not always effective or even feasible for many patients.”
To overcome this challenge, a team of researchers from the UK and USA tested whether, rather than asking patients to contaminate their own hands, it might be possible to help them overcome their fears by contaminating a fake hand instead – a procedure they call ‘multisensory stimulation therapy’.
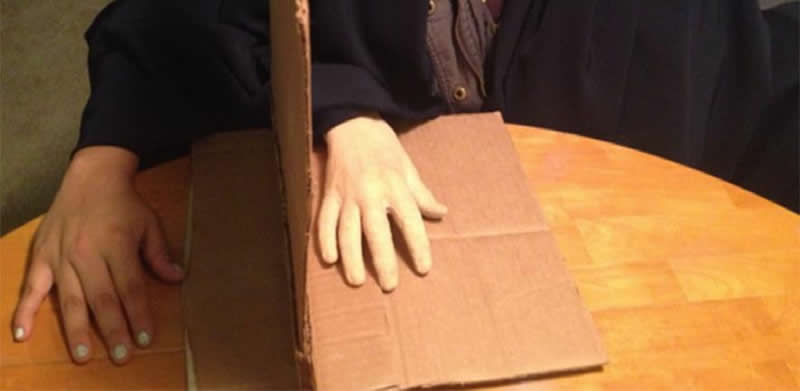
The technique builds on a famous trick known as the ‘rubber hand illusion’. In this illusion, an individual places both hands in front of them on a table, either side of a partition such that they cannot see their right hand. Instead, to the left of the partition they see a fake right hand. The illusionist – in this case, the experimenter – strokes both the fake hand and hidden right hand using a paintbrush. After several minutes of stroking the individual often reports ‘feeling’ touch arising from the fake hand as though it was their own.
In the majority of cases, the rubber hand illusion only works if both hands are stroked in synchrony; if they are stroked asynchronously, the illusion is diminished or disappears entirely. However, in a number of psychiatric conditions such as schizophrenia and body dysmorphic disorder, the illusion appears to work in both cases, suggesting that the body image held in the minds of these patients is more malleable than in healthy individuals.
In a previous study, carried out by Jalal and neuroscientist VS Ramachandran using healthy volunteers, once the illusion had begun to work, the researchers contaminated the dummy hand with fake faeces. The participants reported disgust sensations as if it were their own hand that had been contaminated.
In a new study published today in Frontiers in Human Neuroscience, Jalal and Ramachandran teamed up with researchers at Harvard University – Richard J McNally, Director of Clinical Training in Department Psychology and Jason A Elias and Sriramya Potluri in the Department Psychiatry.
The team recruited 29 OCD patients from the McLean Hospital Obsessive Compulsive Disorder Institute, an intensive residential treatment programme affiliated with Harvard Medical School. Sixteen of these patients had their hidden and dummy hands stroked at the same time, while the remaining 13 patients (the control group) had their hands stroked out of synch.
After 5 minutes of stroking, the participant was asked to rate how much the rubber hand felt like their own. The experimenter then used a tissue to smear the fake faeces on the rubber hand while simultaneously dabbing a damp paper towel on the participant’s real right hand (to create the sensation of having the contaminant smeared on their real hand). The participant was then asked to rate their disgust, anxiety and handwashing urge levels, and the experimenter rated the participant’s facial expression of disgust.
The researchers found that patients in both the experimental and control groups felt an equally strong rubber hand illusion. In other words, even when their real and fake hands were being stroked asynchronously, they had still begun to sense the fake hand as their own. Unsurprisingly, therefore, patients in both groups initially reported similar levels of contamination.
The experimenter then removed the clean paper towel and the tissue that had been used to contaminate the rubber hand, leaving fake faeces on the rubber hand. The experimenter continued to stroke the rubber hand and the participant’s real hand for an additional 5 minutes, after which the participant again provided contamination ratings and the experimenter rated their facial expression.
Now, the patients in the experimental condition were more disgusted: 65% of participants in the experimental condition had a disgust facial expression compared to 35% in the control. This supports previous studies that show that the rubber hand illusion becomes stronger the longer the hand is stroked.
Next, the experimenter stopped the stroking and placed the fake faeces on the patient’s real, right hand and asked the participant once again to provide contamination ratings. Now the differences were much more pronounced in the experimental condition. While those in the control group had average disgust, anxiety and washing urge levels at nearly 7, the experimental group had levels of nearly 9 – that is, an overall 23% difference in contamination ratings.
“Over time, stroking the real and fake hands in synchrony appears to create a stronger and stronger and stronger illusion to the extent that it eventually felt very much like their own hand,” said Jalal. “This meant that after ten minutes, the reaction to contamination was more extreme. Although this was the point our experiment ended, research has shown that continued exposure leads to a decline in contamination feelings – which is the basis of traditional exposure therapy.”
Jalal says it can be safely assumed that the fake hand contamination procedure would lead to similar fall in levels of disgust and contamination ratings, possibly after 30 minutes.
Jalal says the rubber hand illusion may offer a way of treating OCD patients without the high stress levels that exposure therapy can cause. “If you can provide an indirect treatment that is reasonably realistic, where you contaminate a rubber hand instead of a real hand, this might provide a bridge that will allow more people to tolerate exposure therapy or even to replace exposure therapy altogether.”
Jalal has previously worked on other indirect treatments for treating patients with OCD, including a smartphone app. He says that unlike other indirect treatments, this new approach creates a compelling illusion that a part of the patient’s body is being exposed to contamination and so could be even more immersive. It also has additional benefits: “Whereas traditional exposure therapy can be stressful, the rubber hand illusion often makes people laugh at first, helping put them at ease. It is also straightforward and cheap compared to virtual reality, and so can easily reach patients in distress no matter where they are, such as poorly resourced and emergency settings.”
Jalal says the next step is to do randomised clinical trials and compare this technique to existing treatments. Ramachandran agrees, adding: “These results are compelling but not conclusive. We need larger samples and to iron out some methodological wrinkles.”
Other applications of multisensory stimulation therapy might include therapy for people afraid of needles. Exposure therapy would mean repeated needle injections into a real arm and could result in punctured veins. Using a fake hand could provide a clever and convenient alternative.
Source:
University of Cambridge
Media Contacts:
Craig Brierley – University of Cambridge
Image Source:
The image is credited to University of Cambridge.
Original Research: Open access
““Fake it till You Make it”! Contaminating Rubber Hands (“Multisensory Stimulation Therapy”) to Treat Obsessive-Compulsive Disorder”. Baland Jalal et al.
Frontiers in Neuroscience doi:10.3389/fnhum.2019.00414.
Abstract
“Fake it till You Make it”! Contaminating Rubber Hands (“Multisensory Stimulation Therapy”) to Treat Obsessive-Compulsive Disorder
Obsessive-compulsive disorder (OCD) is a deeply enigmatic psychiatric condition associated with immense suffering worldwide. Efficacious therapies for OCD, like exposure and response prevention (ERP), are sometimes poorly tolerated by patients. As many as 25% of patients refuse to initiate ERP mainly because they are too anxious to follow exposure procedures. Accordingly, we proposed a simple and tolerable (immersive yet indirect) low-cost technique for treating OCD that we call “multisensory stimulation therapy.” This method involves contaminating a rubber hand during the so-called “rubber hand illusion” (RHI) in which tactile sensations may be perceived as arising from a fake hand. Notably, Jalal et al. (2015) showed that such fake hand contamination during the RHI provokes powerful disgust reactions in healthy volunteers. In the current study, we explored the therapeutic potential of this novel approach. OCD patients (n = 29) watched as their hidden real hand was being stroked together with a visible fake hand; either synchronously (inducing the RHI; i.e., the experimental condition; n = 16) or asynchronously (i.e., the control condition; n = 13). After 5 min of tactile stimulation, the rubber hand was contaminated with fake feces, simulating conventional exposure therapy. Intriguingly, results suggested sensory assimilation of contamination sensations into the body image via the RHI: patients undergoing synchronous stimulation did not report greater contamination sensations when the fake hand was initially contaminated relative to asynchronous stroking. But contrary to expectations, they did so after the rubber hand had been contaminated for 5 min, as assessed via disgust facial expressions (a secondary outcome) and in vivo exposure (upon discontinuing the illusion). Further, to our surprise, synchronous and asynchronous stroking induced an equally vivid and fast-emerging illusion, which helps explain why both conditions initially (5 min after initiating tactile stimulation) provoked contamination reactions of equal magnitude. This study is the first to suggest heightened malleability of body image in OCD. Importantly, it may pave the way for a tolerable technique for the treatment of OCD—highly suitable for poorly resourced and emergency settings, including low-income and developing countries with minimal access to high-tech solutions like virtual reality.




