Summary: Researchers report a thrombectomy can benefit people up to 7.3 hours following a stroke.
Source: UCLA.
UCLA-led study shows that stent retrievers can provide benefits more than seven hours after onset.
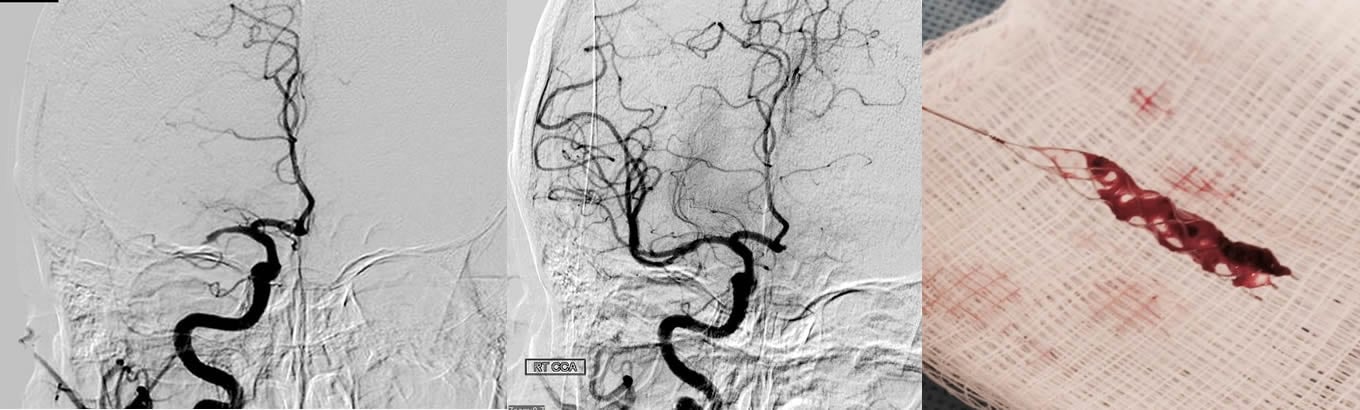
Time is of the essence when getting people stricken with acute ischemic strokes to treatment. And the use of stent retrievers — devices that remove the blood clot like pulling a cork out of a wine bottle — has proven to be a breakthrough for removing the life-threatening blockage of blood flow to the brain.
Current professional guidelines recommend that the procedure be performed within six hours for people to benefit. But researchers on a UCLA-led study published today in the Journal of the American Medical Association have found that the procedure has benefits for people up to 7.3 hours following the onset of a stroke.
“Extending the time window for therapy will let us help more patients, including patients who were not able to get to a hospital right away because the stroke started while they were asleep or made them unable to call for help,” said Dr. Jeffrey Saver, director of the UCLA Comprehensive Stroke Center and the study’s lead author.
The researchers also found that for each six-minute delay, there is a 1 percent increase in the proportion of people who end up disabled, underscoring the need for people to seek treatment as quickly as possible when they experience symptoms of a stroke. The study examined the relationship between the onset of the stroke, the amount of time until the blockage was treated and patient outcomes.
The first coil-shaped clot retriever was invented at UCLA and cleared for use in 2004. For this study, researchers primarily used a newer generation of stent retrievers, which were cleared for use in 2012. First, doctors insert the small mesh tubes through an artery in the leg to the blockage in the artery that takes blood to the brain. Next, they open the mesh tubes in the middle of the clot and then extract the stent and the clot to restore blood flow to the brain.
The current study combines data from five clinical trials involving a total of 1,287 people, including the SWIFT PRIME trial led by Saver, that show these devices improved outcomes for people with acute ischemic strokes due to large vessel blockage. The researchers analyzed the relationship between time from onset of the blockage to treatment and outcome among these patients.
The researchers found that people treated earlier with the retrievers plus standard medical therapy were less likely to be disabled three months after surgery than people who only received medical therapy. Outcomes were the best if the procedure was done within the first two hours of a stroke, but those treated up to 7.3 hours after a stroke continued to show a lesser benefit.
Earlier treatment is better than later treatment to restore blood flow and prevent or limit damage to the brain, Saver noted.
“It is important for the public to know the critically important relationship between time to treatment and outcome, so they know to activate the 911 system as soon as possible when they detect stroke symptoms in themselves or friends, family and co-workers,” he said. “And it is important to reorganize regional systems of stroke care to ensure that ambulances transport appropriate patients to hospitals that perform this procedure quickly and safely.”
The people in these trials were seen at mostly academic medical centers, so the question remains as to whether these same results can be achieved at non-academically affiliated medical centers. Other elements that could skew the results include differences in trial entry criteria and patient characteristics, and that these results may not apply to people who did not qualify for the trials.
In future studies, the researchers plan to use brain imaging techniques to determine if it is possible to identify a specific, smaller group of people who can benefit from the clot retrieval therapy seven to 24 hours after stroke onset, said Dr. Reza Jahan, professor of radiology and neurosurgery at UCLA, and a co-author of the study.
The five trials were funded by European and Canadian government agencies and by companies that make retrieval devices. This pooled analysis was funded by Medtronic, a maker of the retriever devices. The funding went to the University of Calgary, which collaborated on this study.
Funding: Saver reports that he has received study funding in the past from Medtronic, Stryker and Neuravia. The Regents of the University of California have intellectual property rights in stent retrievers.
Source: Enrique Rivero – UCLA
Image Source: This NeuroscienceNews.com image is credited May Nour, MD.
Original Research: Full open access research for “Time to Treatment With Endovascular Thrombectomy and Outcomes From Ischemic Stroke: A Meta-analysis” by Jeffrey L. Saver, MD; Mayank Goyal, MD; Aad van der Lugt, MD; Bijoy K. Menon, MD; Charles B. L. M. Majoie, MD; Diederik W. Dippel, MD; Bruce C. Campbell, MD, PhD; Raul G. Nogueira, MD; Andrew M. Demchuk, MD; Alejandro Tomasello, MD; Pere Cardona, MD; Thomas G. Devlin, MD; Donald F. Frei, MD; Richard du Mesnil de Rochemont, MD; Olvert A. Berkhemer, MD; Tudor G. Jovin, MD; Adnan H. Siddiqui, MD, PhD; Wim H. van Zwam, MD; Stephen M. Davis, MD; Carlos Castaño, MD; Biggya L. Sapkota, MD; Puck S. Fransen, MD; Carlos Molina, MD; Robert J. van Oostenbrugge, MD; Ángel Chamorro, MD; Hester Lingsma, PhD; Frank L. Silver, MD; Geoffrey A. Donnan, MD; Ashfaq Shuaib, MD; Scott Brown, PhD; Bruce Stouch, PhD; Peter J. Mitchell, MD; Antoni Davalos, MD; Yvo B. W. E. M. Roos, MD; Michael D. Hill, MD, MS; for the HERMES Collaborators in JAMA. Published online September 27 2016 doi:10.1001/jama.2016.13647
[cbtabs][cbtab title=”MLA”]UCLA. “Time Window to Help Stroke Patients Longer Than Previously Thought.” NeuroscienceNews. NeuroscienceNews, 28 September 2016.
<https://neurosciencenews.com/stroke-neurology-time-frame-5148/>.[/cbtab][cbtab title=”APA”]UCLA. (2016, September 28). Time Window to Help Stroke Patients Longer Than Previously Thought. NeuroscienceNews. Retrieved September 28, 2016 from https://neurosciencenews.com/stroke-neurology-time-frame-5148/[/cbtab][cbtab title=”Chicago”]UCLA. “Time Window to Help Stroke Patients Longer Than Previously Thought.” https://neurosciencenews.com/stroke-neurology-time-frame-5148/ (accessed September 28, 2016).[/cbtab][/cbtabs]
Abstract
Time to Treatment With Endovascular Thrombectomy and Outcomes From Ischemic Stroke: A Meta-analysis
Importance Endovascular thrombectomy with second-generation devices is beneficial for patients with ischemic stroke due to intracranial large-vessel occlusions. Delineation of the association of treatment time with outcomes would help to guide implementation.
Objective To characterize the period in which endovascular thrombectomy is associated with benefit, and the extent to which treatment delay is related to functional outcomes, mortality, and symptomatic intracranial hemorrhage.
Design, Setting, and Patients Demographic, clinical, and brain imaging data as well as functional and radiologic outcomes were pooled from randomized phase 3 trials involving stent retrievers or other second-generation devices in a peer-reviewed publication (by July 1, 2016). The identified 5 trials enrolled patients at 89 international sites.
Exposures Endovascular thrombectomy plus medical therapy vs medical therapy alone; time to treatment.
Main Outcomes and Measures The primary outcome was degree of disability (mRS range, 0-6; lower scores indicating less disability) at 3 months, analyzed with the common odds ratio (cOR) to detect ordinal shift in the distribution of disability over the range of the mRS; secondary outcomes included functional independence at 3 months, mortality by 3 months, and symptomatic hemorrhagic transformation.
Results Among all 1287 patients (endovascular thrombectomy + medical therapy [n = 634]; medical therapy alone [n = 653]) enrolled in the 5 trials (mean age, 66.5 years [SD, 13.1]; women, 47.0%), time from symptom onset to randomization was 196 minutes (IQR, 142 to 267). Among the endovascular group, symptom onset to arterial puncture was 238 minutes (IQR, 180 to 302) and symptom onset to reperfusion was 286 minutes (IQR, 215 to 363). At 90 days, the mean mRS score was 2.9 (95% CI, 2.7 to 3.1) in the endovascular group and 3.6 (95% CI, 3.5 to 3.8) in the medical therapy group. The odds of better disability outcomes at 90 days (mRS scale distribution) with the endovascular group declined with longer time from symptom onset to arterial puncture: cOR at 3 hours, 2.79 (95% CI, 1.96 to 3.98), absolute risk difference (ARD) for lower disability scores, 39.2%; cOR at 6 hours, 1.98 (95% CI, 1.30 to 3.00), ARD, 30.2%; cOR at 8 hours,1.57 (95% CI, 0.86 to 2.88), ARD, 15.7%; retaining statistical significance through 7 hours and 18 minutes. Among 390 patients who achieved substantial reperfusion with endovascular thrombectomy, each 1-hour delay to reperfusion was associated with a less favorable degree of disability (cOR, 0.84 [95% CI, 0.76 to 0.93]; ARD, −6.7%) and less functional independence (OR, 0.81 [95% CI, 0.71 to 0.92], ARD, −5.2% [95% CI, −8.3% to −2.1%]), but no change in mortality (OR, 1.12 [95% CI, 0.93 to 1.34]; ARD, 1.5% [95% CI, −0.9% to 4.2%]).
Conclusions and Relevance In this individual patient data meta-analysis of patients with large-vessel ischemic stroke, earlier treatment with endovascular thrombectomy + medical therapy compared with medical therapy alone was associated with lower degrees of disability at 3 months. Benefit became nonsignificant after 7.3 hours.
“Time to Treatment With Endovascular Thrombectomy and Outcomes From Ischemic Stroke: A Meta-analysis” by Jeffrey L. Saver, MD; Mayank Goyal, MD; Aad van der Lugt, MD; Bijoy K. Menon, MD; Charles B. L. M. Majoie, MD; Diederik W. Dippel, MD; Bruce C. Campbell, MD, PhD; Raul G. Nogueira, MD; Andrew M. Demchuk, MD; Alejandro Tomasello, MD; Pere Cardona, MD; Thomas G. Devlin, MD; Donald F. Frei, MD; Richard du Mesnil de Rochemont, MD; Olvert A. Berkhemer, MD; Tudor G. Jovin, MD; Adnan H. Siddiqui, MD, PhD; Wim H. van Zwam, MD; Stephen M. Davis, MD; Carlos Castaño, MD; Biggya L. Sapkota, MD; Puck S. Fransen, MD; Carlos Molina, MD; Robert J. van Oostenbrugge, MD; Ángel Chamorro, MD; Hester Lingsma, PhD; Frank L. Silver, MD; Geoffrey A. Donnan, MD; Ashfaq Shuaib, MD; Scott Brown, PhD; Bruce Stouch, PhD; Peter J. Mitchell, MD; Antoni Davalos, MD; Yvo B. W. E. M. Roos, MD; Michael D. Hill, MD, MS; for the HERMES Collaborators in JAMA. Published online September 27 2016 doi:10.1001/jama.2016.13647