Study links enlarged brain cavities to need for second surgery after birth.
Fetuses with enlarged ventricles—the fluid-filled cavities inside the brain—may be less likely than other fetuses to benefit from surgery in the womb to treat spina bifida, according to a study co-authored by researchers at UCSF Benioff Children’s Hospital San Francisco.
The researchers found that fetuses with enlarged ventricles were more likely to require a second surgery to relieve a life-threatening build-up of pressure within the brain. Given the risks that fetal surgery poses for mother and newborn, the findings indicate that in these cases, it may be better to wait until after birth to perform the corrective spinal surgery. The scientists made this discovery by analyzing data from the 2011 Management of Myelomeningocele (MOMS) study, led by UCSF. In the multicenter MOMS study, the researchers reported that surgically correcting the spinal defect while the fetus is in the womb greatly reduced the need to divert, or shunt, fluid away from the ventricles to relieve hydrocephalus, the life-threatening buildup of pressure inside the skull that sometimes accompanies myelomeningocele.
“Currently, we offer this surgery after extensive counseling and evaluation, and patients have to weigh the risks of open fetal surgery versus the potential benefit that is seen in some babies but not others. This is a grueling decision for parents to have to make because the flipside of doing the surgery is the risk of prematurity,” said co-author Larry Rand, MD, director of perinatal services at the UCSF Fetal Treatment Center at UCSF Benioff Children’s Hospital San Francisco.
“Until now, there hasn’t been a clear criteria to predict who is most likely to benefit from the surgery and who is most likely to go into preterm labor. This study is the first major follow up to the initial MOMS trial and provides direction about the likelihood of benefiting from the surgery based on the findings on prenatal scans,” said Rand.
The study appears in the October issue of the Journal of Neurosurgery: Pediatrics. It was led by Noel Tulipan, MD of Vanderbilt University Medical Center with N. Scott Adzick, MD, of the Children’s Hospital of Philadelphia as senior author.
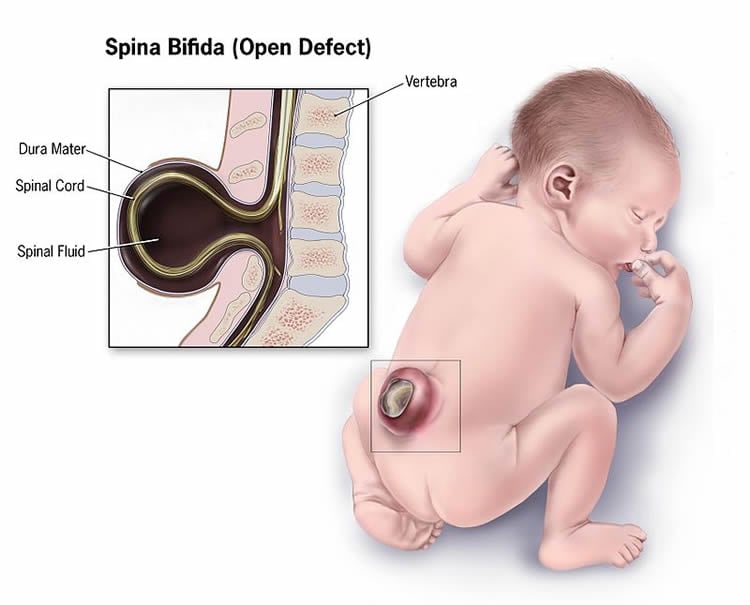
Spina bifida arises during the first few weeks of development when the neural tube – the embryonic structure that ultimately becomes the central nervous system – fails to close, resulting in an underdeveloped spinal cord.
In cases of myelomeningocele, a portion of the spinal cord is left exposed and protrudes through an opening on the baby’s back that resembles a cyst. Children with myelomeningocele face lifelong disabilities including leg weakness or paralysis and a loss of bladder and bowel control. They often need braces to walk or are wheelchair-bound.
In the current analysis of data from the original MOMS study, the researchers found that fetuses who had larger ventricles were equally as likely to require placement of a shunt during the first year after birth, regardless of when they underwent the spinal repair surgery.
The original MOMS study found that infants who had undergone the surgery before birth were more likely to walk without crutches or other devices. At 30 months of age, the fetal surgery group also had higher scores in tests of mental and motor development. However, as with any surgery, the procedure presented risks. Babies who underwent surgery in the uterus were more likely to be born preterm than were those who had the surgery after birth. Additionally, mothers in the fetal surgery group were at risk for having the surgical scar on the uterus tear or rupture during subsequent pregnancies.
The surgical procedures evaluated in the MOMS trial were developed at the UCSF Fetal Treatment Center under the direction of Michael Harrison, MD, a UCSF professor emeritus considered the “Father of Fetal Surgery.” UCSF researchers performed the pioneering animal studies in the 1990’s that established a rationale for treating spina bifida – the first nonfatal condition treated at the Center – before birth. Already the world leader in diagnosing and treating birth defects in utero, UCSF became the first institution to successfully perform fetal surgery in 1981 and has trained most of the current leaders in the field.
In the current analysis, researchers tabulated the results in a single, composite outcome, to highlight the differences between treatment and control groups. The primary combined outcome for this analysis was whether a child had died, had a shunt placed in the first year after birth, or met the study’s criteria for when to place a shunt.
Of the women who took part in the study, 91 were randomized to the prenatal surgery group and 92 to the postnatal group. Of these, 72.5 percent in the prenatal surgery group and 97.8 percent in the postnatal surgery group met the criteria for inclusion in the primary outcome. Overall, 44 percent of children in the prenatal surgery group had a shunt placed, compared to 83.7 percent in the postnatal group.
When the women were first enrolled in the MOMS study, they had fetal imaging as part of the evaluation. Exact ventricle size was then determined with magnetic resonance imaging scans of the fetuses’ brains.
Irrespective of whether they were in the prenatal or postnatal surgery group, children with the largest ventricles were more likely to require a shunt than those with smaller ventricles. For the prenatal surgery group, shunts were eventually placed in 20 percent of those with ventricles less than 10 mm required a shunt, 45.2 percent with ventricles from 10 to just below 15 mm, and 79 percent with ventricle size of 15 mm or greater. For the postnatal surgery group, shunts were placed in 79.4 percent, 86 percent, and 87.5 percent, respectively.
The researchers concluded that fetuses with ventricles smaller than 10 mm are the ideal candidates for fetal surgery, while there appears to be no benefit, in relation to shunting, for fetuses with ventricles 15 mm or larger. Cases in between should be evaluated carefully before deciding whether to refer them for fetal surgery, the authors wrote.
Funding: The study was supported by grants from the Eunice Kennedy Shriver National Institute of Child and Health and Human Development. Other institutions involved in the research include George Washington University and Columbia University.
Source: Juliana Bunim – UCSF
Image Source: The image is credited to the CDC and is in the public domain
Original Research: Abstract for “Prenatal surgery for myelomeningocele and the need for cerebrospinal fluid shunt placement” by Noel Tulipan, MD, John C. Wellons III, MD, MSPH, Elizabeth A. Thom, PhD, Nalin Gupta, MD, PhD, Leslie N. Sutton, MD, Pamela K. Burrows, MS, Diana Farmer, MD, William Walsh, MD, Mark P. Johnson, MD, Larry Rand, MD, Susan Tolivaisa, BS, Mary E. D’alton, MD, and N. Scott Adzick, MD for the MOMS Investigators in Journal of Neurosurgery: Pediatrics. Published online September 15 2015 doi:10.3171/2015.7.PEDS15336
Abstract
Prenatal surgery for myelomeningocele and the need for cerebrospinal fluid shunt placement
OBJECT
The Management of Myelomeningocele Study (MOMS) was a multicenter randomized trial comparing the safety and efficacy of prenatal and postnatal closure of myelomeningocele. The trial was stopped early because of the demonstrated efficacy of prenatal surgery, and outcomes on 158 of 183 pregnancies were reported. Here, the authors update the 1-year outcomes for the complete trial, analyze the primary and related outcomes, and evaluate whether specific prerandomization risk factors are associated with prenatal surgery benefit.
METHODS
The primary outcome was a composite of fetal loss or any of the following: infant death, CSF shunt placement, or meeting the prespecified criteria for shunt placement. Primary outcome, actual shunt placement, and shunt revision rates for prenatal versus postnatal repair were compared. The shunt criteria were reassessed to determine which were most concordant with practice, and a new composite outcome was created from the primary outcome by replacing the original criteria for CSF shunt placement with the revised criteria. The authors used logistic regression to estimate whether there were interactions between the type of surgery and known prenatal risk factors (lesion level, gestational age, degree of hindbrain herniation, and ventricle size) for shunt placement, and to determine which factors were associated with shunting among those infants who underwent prenatal surgery.
RESULTS
Ninety-one women were randomized to prenatal surgery and 92 to postnatal repair. The primary outcome occurred in 73% of infants in the prenatal surgery group and in 98% in the postnatal group (p < 0.0001). Actual rates of shunt placement were only 44% and 84% in the 2 groups, respectively (p < 0.0001). The authors revised the most commonly met criterion to require overt clinical signs of increased intracranial pressure, defined as split sutures, bulging fontanelle, or sunsetting eyes, in addition to increasing head circumference or hydrocephalus. Using these modified criteria, only 3 patients in each group met criteria but did not receive a shunt. For the revised composite outcome, there was a difference between the prenatal and postnatal surgery groups: 49.5% versus 87.0% (p < 0.0001). There was also a significant reduction in the number of children who had a shunt placed and then required a revision by 1 year of age in the prenatal group (15.4% vs 40.2%, relative risk 0.38 [95% CI 0.22–0.66]). In the prenatal surgery group, 20% of those with ventricle size < 10 mm at initial screening, 45.2% with ventricle size of 10 up to 15 mm, and 79.0% with ventricle size ≥ 15 mm received a shunt, whereas in the postnatal group, 79.4%, 86.0%, and 87.5%, respectively, received a shunt (p = 0.02). Lesion level and degree of hind-brain herniation appeared to have no effect on the eventual need for shunting (p = 0.19 and p = 0.13, respectively). Similar results were obtained for the revised outcome.
CONCLUSIONS
Larger ventricles at initial screening are associated with an increased need for shunting among those undergoing fetal surgery for myelomeningocele. During prenatal counseling, care should be exercised in recommending prenatal surgery when the ventricles are 15 mm or larger because prenatal surgery does not appear to improve outcome in this group. The revised criteria may be useful as guidelines for treating hydrocephalus in this group.
“Prenatal surgery for myelomeningocele and the need for cerebrospinal fluid shunt placement” by Noel Tulipan, MD, John C. Wellons III, MD, MSPH, Elizabeth A. Thom, PhD, Nalin Gupta, MD, PhD, Leslie N. Sutton, MD, Pamela K. Burrows, MS, Diana Farmer, MD, William Walsh, MD, Mark P. Johnson, MD, Larry Rand, MD, Susan Tolivaisa, BS, Mary E. D’alton, MD, and N. Scott Adzick, MD for the MOMS Investigators in Journal of Neurosurgery: Pediatrics. Published online September 15 2015 doi:10.3171/2015.7.PEDS15336