Summary: The remnants of the Lyme causing B. burgdorferi bacteria may be responsible for the neuroinflammation associated with long-term Lyme disease symptoms. Researchers say the remnants are more inflammatory than the live bacteria.
Source: Tulane University
Even after antibiotic treatment, some Lyme disease patients suffer from an array of symptoms including neurological issues that greatly diminish their quality of life. Brain scans of these patients show persistent neuroinflammation, but the cause has been unclear.
Tulane University researchers have discovered that remnants of B. burgdorferi, the bacteria that causes Lyme disease, may contribute to inflammation in both the central and peripheral nervous systems.
These remnants are significantly more inflammatory than live, intact bacteria published in Scientific Reports.
Lead researcher Geetha Parthasarathy, Ph.D., assistant professor of immunology at the Tulane National Primate Research Center, explored the effects of B. burgdorferi remnants on nervous system tissue using a nonhuman primate model, investigating the effects on both the frontal cortex and dorsal root ganglion.
Inflammatory markers in these areas were several times higher in samples exposed to remnants of B. burgdorferi than in samples exposed to live bacteria, and several times higher in the frontal cortex than the dorsal root ganglion. The bacterial remnants also caused cell death in brain neurons.
“As neuroinflammation is the basis of many neurological disorders, lingering inflammation in the brain due to these unresolved fragments could cause long term health consequences,” Parthasarathy said.
Scientists still don’t know how B. burgdorferi spirochetes find their way into brain tissue. In longstanding or persistent Lyme disease infections, bacterial spirochetes may harbor inside major organs including the heart and brain, where they could continue to wreak havoc over time. Antibiotics may kill the bacteria in these organs, but remnants could remain if the body cannot adequately eliminate them.
Parthasarathy said the findings may explain some of the neurological symptoms and conditions that patients with persistent Lyme infections can experience. She plans future studies to investigate new anti-inflammatory therapies for antibiotic-resistant neuroinflammation and to explore why the body may not be clearing these bacterial remnants.
About this neurology research news
Author: Leslie Tate
Source: Tulane University
Contact: Leslie Tate – Tulane University
Image: The image is credited to the researchers
Original Research: Open access.
“Neuropathogenicity of non-viable Borrelia burgdorferi ex vivo” by Geetha Parthasarathy et al. Scientific Reports
Abstract
Neuropathogenicity of non-viable Borrelia burgdorferi ex vivo
Even after appropriate treatment, a proportion of Lyme disease patients suffer from a constellation of symptoms, collectively called Post-Treatment Lyme Disease Syndrome (PTLDS). Brain PET scan of patients with PTLDS have demonstrated likely glial activation indicating persistent neuroinflammatory processes.
It is possible that unresolved bacterial remnants can continue to cause neuroinflammation. In previous studies, we have shown that non-viable Borrelia burgdorferi can induce neuroinflammation and apoptosis in an oligodendrocyte cell line.
In this follow-up study, we analyze the effect of sonicated remnants of B. burgdorferi on primary rhesus frontal cortex (FC) and dorsal root ganglion (DRG) explants. Five FC and three DRG tissue fragments from rhesus macaques were exposed to sonicated B. burgdorferi and analyzed for 26 inflammatory mediators. Live bacteria and medium alone served as positive and negative control, respectively.
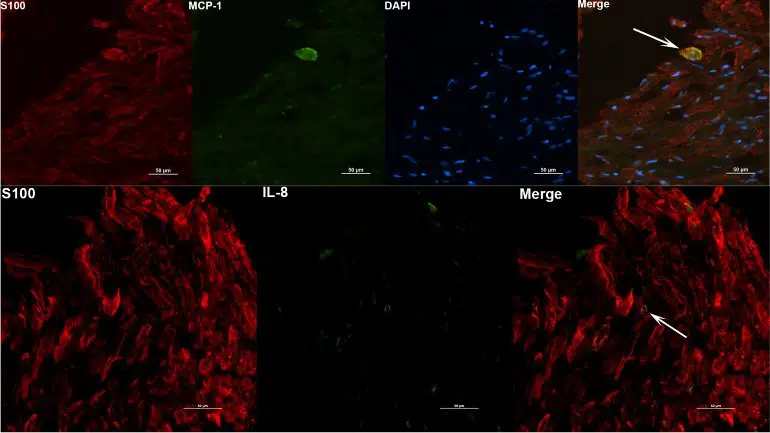
Tissues were also analyzed for cell types mediating inflammation and overall apoptotic changes. Non-viable B. burgdorferi induced significant levels of several inflammatory mediators in both FC and DRG, similar to live bacteria. However, the levels induced by non-viable B. burgdorferi was often (several fold) higher than those induced by live ones, especially for IL-6, CXCL8 and CCL2. This effect was also more profound in the FC than in the DRG. Although the levels often differed, both live and dead fragments induced the same mediators, with significant overlap between FC and DRG. In the FC, immunohistochemical staining for several inflammatory mediators showed the presence of multiple mediators in astrocytes, followed by microglia and oligodendrocytes, in response to bacterial remnants.
Staining was also seen in endothelial cells. In the DRG, chemokine/cytokine staining was predominantly seen in S100 positive (glial) cells. B. burgdorferi remnants also induced significant levels of apoptosis in both the FC and DRG. Apoptosis was confined to S100 + cells in the DRG while distinct neuronal apoptosis was also detected in most FC tissues in response to sonicated bacteria. Non-viable B. burgdorferi can continue to be neuropathogenic to both CNS and PNS tissues with effects likely more profound in the former.
Persistence of remnant-induced neuroinflammatory processes can lead to long term health consequences.