Summary: Anti-Drebrin auto-antibodies may be responsible for limbic encephalitis.
Source: University of Bonn
Certain forms of epilepsy are accompanied by inflammation of important brain regions. Researchers at the University of Bonn have now identified a mechanism that explains this link. Their results may also pave the way to new therapeutic options in the medium term. They have now been published in the renowned scientific journal “Annals of Neurology”.
Epilepsy can be hereditary. In other cases, patients only develop the disease later in life: as a result of a brain injury, after a stroke or triggered by a tumor. Inflammation of the meninges or the brain itself can also result in epilepsy.
Particularly dangerous are inflammatory reactions affecting the hippocampus, a brain structure that plays an important role in memory processes and the development of emotions. Doctors call this condition limbic encephalitis. “However, in many cases it is still not clear what causes such inflammation,” explains Prof. Dr. Albert Becker, who heads the Section for Translational Epilepsy Research at the University Hospital Bonn.
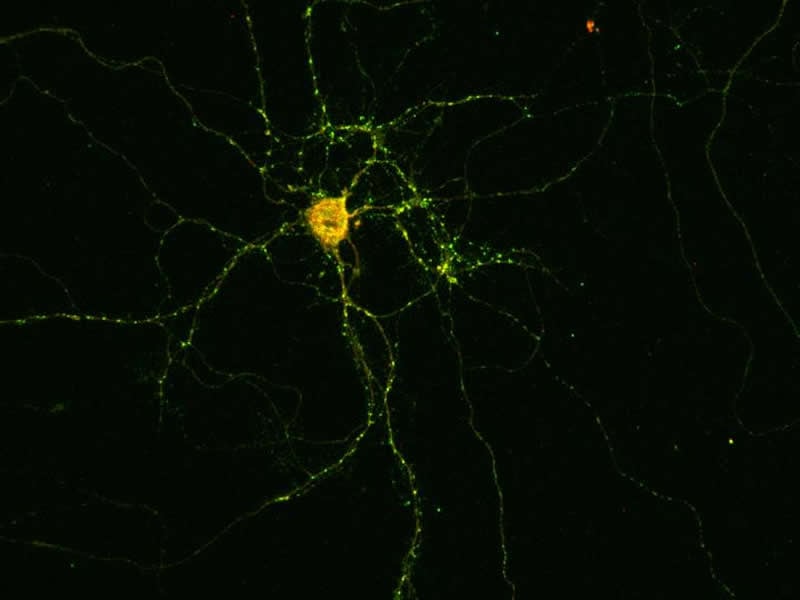
Researchers have now identified an autoantibody that is believed to be responsible for encephalitis in some patients. Unlike normal antibodies, it is not directed against molecules that have entered the organism from outside, but against the body’s own structures – hence the prefix “auto”, which can be translated as “self”. The researchers discovered it in the spinal fluid of epilepsy patients suffering from acute inflammation of the hippocampus. The autoantibody is directed against the protein Drebrin. Drebrin ensures that the contact points between nerve cells function correctly. At these so-called synapses, the neurons are interconnected and pass on their information.
When the autoantibody encounters a Drebrin molecule, it knocks it out of action and thereby disrupts the transmission of information between nerve cells. At the same time, it alerts the immune system, which is then activated and switches to an inflammatory mode, while simultaneously producing even more autoantibodies. “However, Drebrin is located inside the synapses, whereas the autoantibody is located in the tissue fluid,” says Dr. Julika Pitsch, who heads a junior research group in Prof. Becker’s department. “These two should therefore normally never come into contact with each other.” The autoantibody seems to use a back door to enter the cell. This is actually intended for completely different molecules: the so-called neurotransmitters.
Into the nerve cell by Trojan horse
Information processing in the brain is electrical. The synapses themselves, however, communicate via chemical messengers, the aforementioned neurotransmitters: In response to an electrical pulse, the transmitter synapse emits transmitters that then dock to certain receptors of the receiver synapse, where they in turn also generate electrical pulses.
The synaptic vesicles – the packaging of the neurotransmitters – are absorbed again and recycled. “The autoantibody seems to use this route to sneak into the cell, as with a Trojan horse,” explains Becker’s colleague Prof. Dr. Susanne Schoch McGovern.
In cell culture experiments, the researchers were able to show what happens next: Shortly after the addition of the autoantibody, the neurons in the Petri dish begin to fire machine-gun-like rapid bursts of electrical impulses. “We know that this form of electrical excitation is contagious, so to speak,” emphasizes Prof. Becker. “With nerve cells, which are interconnected to form a network, all the nerve cells involved suddenly start firing wildly.” This may then result in an epileptic seizure.
The results also give hope for new therapeutic approaches. For instance, active substances such as cortisone can suppress the immune system and thereby possibly also prevent the massive production of autoantibodies. It may also be possible to intercept and incapacitate them specifically with certain drugs. But there is still a long way to go before treatment becomes available, stresses Prof. Dr. Rainer Surges, Director of the Department of Epileptology at the University Hospital Bonn. Moreover, it would primarily benefit patients with this particular form of the disease. For them, however, the benefit would probably be huge: In contrast to congenital epilepsies, those based on inflammation may possibly be cured in the future with the appropriate therapy.
Source:
University of Bonn
Media Contacts:
Albert J. Becker – University of Bonn
Image Source:
The image is credited to the AG Becker/Uni Bonn.
Original Research: Open access
“Drebrin autoantibodies in patients with seizures and suspected encephalitis”. Julika Pitsch, Delara Kamalizade, Anna Braun, Julia C. Kuehn, Polina E. Gulakova, Theodor Rueber, Gert Lubec, Dirk Dietrich, Randi von Wrede, Christoph Helmstaedter, Rainer Surges, Christian E. Elger, Elke Hattingen, Hartmut Vatter, Susanne Schoch, Albert J. Becker.
Annals of Neurology doi:10.1002/ana.25720.
Abstract
Drebrin autoantibodies in patients with seizures and suspected encephalitis
Objective
Assess occurrence of the dendritic spine scaffolding protein Drebrin as pathophysiologically relevant autoantibody target in patients with recurrent seizures and suspected encephalitis as leading symptoms.
Methods
Sera of four patients with adult onset epilepsy and suspected encephalitis of unresolved etiology and equivalent results in autoantibody screening were subjected to epitope identification. We combined a wide array of approaches ranging from immunoblotting, immunoprecipitation and mass‐spectrometry, subcellular binding pattern analyses in primary neuronal cultures, immunohistochemistry in brains of wildtype and Drebrin knockout mice to in vitro analyses on impaired synapse formation, morphology and aberrant neuronal excitability by antibody exposure.
Results
In the serum of a patient with adult onset epilepsy and suspected encephalitis, a strong signal at ~70 kDa was detected by immunoblotting, for which mass‐spectrometry revealed Drebrin as putative antigen. Three other patients whose sera also showed strong immunoreactivity around 70 kDa in western blotting were also anti‐Drebrin positive. Seizures, memory impairment and increased protein content in cerebrospinal fluid occurred in anti‐Drebrin seropositive patients. Alterations in cerebral MRI comprised amygdalo‐hippocampal T2‐signal increase and hippocampal sclerosis. Diagnostic biopsy revealed T‐lymphocytic encephalitis in an anti‐Drebrin seropositive patient. Exposure of primary hippocampal neurons to anti‐Drebrin autoantibodies resulted in aberrant synapse composition and Drebrin distribution as well as increased spike rates and the emergence of burst discharges reflecting network hyperexcitability.
Interpretation
Anti‐Drebrin autoantibodies define a chronic syndrome of recurrent seizures, neuropsychiatric impairment as well as inflammation of limbic and occasionally cortical structures. Immunosuppressant therapies should be considered in this disorder.